

More evidence emergences in support of the extended hypothesis of Robert Edgar Hope-Simpson (REHS)
More evidence emergences in support of the extended hypothesis of Robert Edgar Hope-Simpson (REHS)

Recently information has been released online (1), Substack (2) and Youtube (3) that Stanford performed a study investigating whether individuals who tested PCR positive for Covid-19 on entering Stanford Health Care were shedding virus capable of replicating and therefore capable of infecting others. The test procedure that the scientists used for study was an amended PCR test. The PCR test, used routinely through the pandemic, identifies whether a positive RNA strand / sequence is present in the sample. This test procedure examined whether the minus strand was present as the presence of both strands is required for replication and potential infectivity.
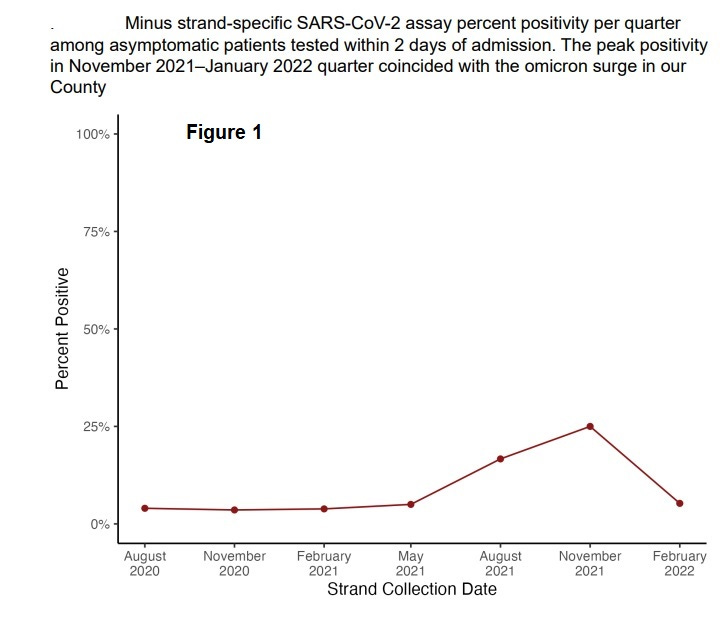
This study was conducted over a significant period (August 2020 to April 2022) and for an extended spell only 4% of people who had a positive PCR test tested positive for the negative stand. There were periods of higher infectivity (see Fig 1). This data is supportive of the REHS extended hypothesis (4) in that the virus embeds within individuals at a low level and then is seasonally reactivated. Reactivated individuals are only briefly highly infectious and barely showing any symptoms. They generate mutations that have the capability to rapidly evade the immune systems of the less healthy and embed within their cells. This rapid entry results in a more severe immune response. This is why they are not infectious and explains the results generated in this study.
It appears that the implications of using a fundamentally flawed test procedure to cancel operations, isolate millions of people and scare individuals out of their minds was buried for at least a year by Stanford as presumably a significant portion of their funding originates from government and big pharma. To date there does not appear to have been publication in a peer reviewed recognised journal which is strange given the importance of these findings. Worse still the CDC published a report in February 2021 on this test and the validation was performed in May – June 2020.
Examining the appendix of the CDC publication (5) it appears that this negative strand test correlates reasonably well with previous publications (6) comparing the ability of Ct values to correlate with the capacity to cultivate live virus and is effectively independent confirmation. For instance, if we take a positive strand PCR test threshold of 26, we find that 37 out of 39 samples tested positive for the negative strand. Only 4 samples tested positive for both strands out of the 105 remaining samples. This indicates that the CDC should have set the PCR Ct threshold at least at around this value.
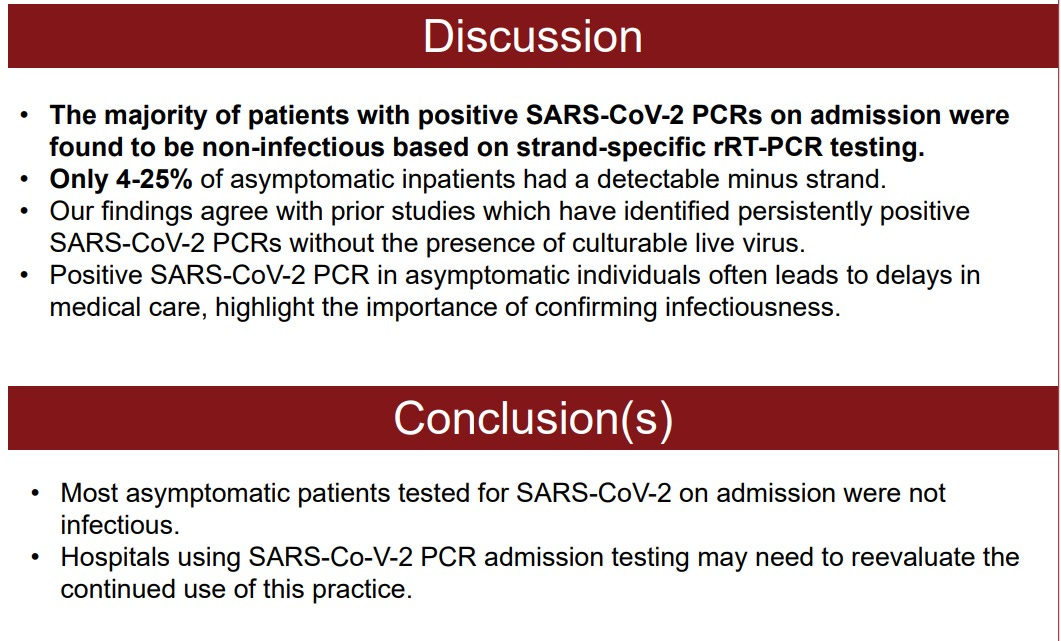
These were the authors discussion and conclusions;
References
(2)

(3)